Health Essentials
Fibroid… Threat to female reproductive health
- /home/u249204778/domains/spectator.com.gh/public_html/wp-content/plugins/mvp-social-buttons/mvp-social-buttons.php on line 27
https://spectator.com.gh/wp-content/uploads/2023/11/A-diagram-on-types-of-fibroids.jpe&description=Fibroid… Threat to female reproductive health', 'pinterestShare', 'width=750,height=350'); return false;" title="Pin This Post">
- Share
- Tweet /home/u249204778/domains/spectator.com.gh/public_html/wp-content/plugins/mvp-social-buttons/mvp-social-buttons.php on line 72
https://spectator.com.gh/wp-content/uploads/2023/11/A-diagram-on-types-of-fibroids.jpe&description=Fibroid… Threat to female reproductive health', 'pinterestShare', 'width=750,height=350'); return false;" title="Pin This Post">
“It is not my time of the month, what is wrong with me,” was the question Setriakor (not her real name) asked herself as she looks at her blood stained dress.
As the days went, the flow was heavier with thick dark clots, for which her usual pad could not sustain. She later resorted to the use of diapers. That also failed to absorb the amount of blood and clots ‘gushing out.’
She dares not laugh, cough or do any strenuous activity, lest her dress will be soiled, wherever she finds herself.
Setriakor, a 36-year old Scripter, looked pale and found it difficult to work for a number of weeks.
She decided to visit a local Chemist to explain her ordeal. In the end, a blood tonic was prescribed for her with the hope to replenish the lost blood.
He also advised her to visit the hospital to see a doctor.
Her visit to the health facility the following week ended up with the gynaecologist who performed a scan on her. The results of the scan revealed she had multiple fibroids.
Suddenly, all the stories she had heard about fibroid began racing through her mind. It took a lot of counselling from the gynaecologist to calm her down.
This is the challenge most young and adult women go through with some either losing their uterus or life in the process due to delay in seeking medical attention.
Fibroid, is non-cancerous growth that develops in or around the womb or uterus. The growth or growths are made up of muscle and fibrous tissue. They vary in size.
Many women are unaware they have fibroids because they do not have any symptoms.
Women who do have symptoms of fibroid are likely to experience heavy or painful periods, abdominal pains, lower back pain, frequent urge to urinate, constipation and pain or discomfort during sex.
Women who are diagnosed of fibroid often undergo hysterectomy in order to have it removed.
Most women of African-Carribean origin tend to develop fibroids more frequently and are common with around one in three women.
Types
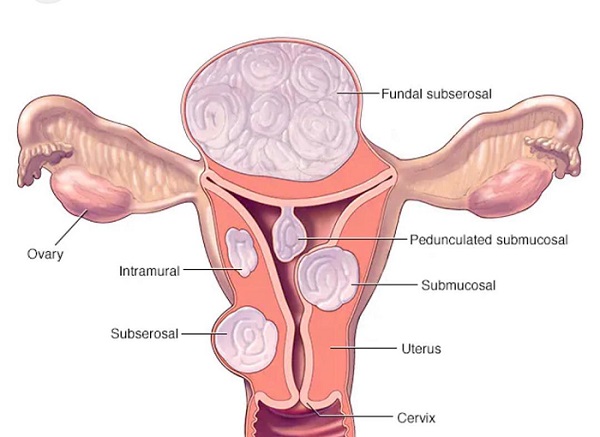
The Chief Executive Officer of Ladybits Health and Wellness Clinic, Dr Victoria Partey-Newman in an interview with The Spectator said there were four types of fibroids which can occur in women.
The types, she said, were intramural, subserosal, submucosal and pendunculated fibroids.
She explained that intramural fibroids occur in the wall of the uterus. This type of fibroid grows quite large.
Subserosal fibroids grow outside the uterus and may press on other organs of the pelvic area.
Submucosal fibroids grow beneath the lining of the uterus and grow into the uterine cavity which is the central part of the uterus.
“Submucosal fibroids can make it harder for one’s uterus to support conception and maintain pregnancy,” Dr Partey-Newman stated.
According to her, submucosal fibroids are most likely to cause painful cramping as well as bleeding between periods.
Pedunculated fibroids are mushroom-like and grows at the end of small stalks within or outside of the uterus. When the stalk of a pedunculated fibroid become twisted, it can cause intense pain.
The uterine fibroids, however, are the most common tumour in women and very prevalent in infertility issues.
Infertility
Dr Partey-Newman said fibroids could be the sole cause of infertility in two to three per cent of women but the exact cause is unknown. It has often been linked to the hormone oestrogen.
Oestrogen is the female reproductive hormone produced by the ovaries.
Dr Partey-Newman said fibroids most often develop between the start of puberty and menopause, adding that the risk increases with age.
According to her, having a family member with fibroids could increase one’s risk of having it but said “you should not discount the symptoms simply because you do not have a family member with fibroids.”
She said fibroids cannot be prevented but can reduce risk by maintaining a healthy body weight and have a regular pelvic examinations.
Treatment
Dr Partey-Newman said surgery was not the only option for the treatment of fibroids.
They can be treated with medication.
Currently, Gonadotrophin-releasing hormone (GnRH) agonists and selective progesterone receptor modulators (SPRMs) are the most effective medical therapies with the most evidence to support the reduction of fibroid volume in menstrual bleeding.
Another way to treat fibroid was uterine fibroid embolisation which is done by cutting off blood supply to the fibroids. That causes them to shrink.
Dr Partey-Newman, however, said “if symptoms do not improve with medication or nonsurgical treatment, or if the gynaecologist suspects fibroids may be causing infertility, surgery may be the next treatment option.
“The goal of surgery may be to relieve pain, reduce menstrual blood flow, or improve fertility.”
Advice
She said since fibroids could reoccur after surgery, it was important for women to quickly get married and start making babies, especially those who have had their fibroids removed.
“In our society, where men are the ones that propose mostly, it somehow makes it difficult for women to marry early and start giving birth.
That contributes in making the fibroids recur again.
She advised women to visit the hospital when they notice changes in their reproductive cycle and urged them to adhere to doctor’s advice when diagnosed of the disease.
She cautioned that women diagnosed of fibroids must avoid herbal concoctions which could affect their kidneys in the long term.
By Jemima Esinam Kuatsinu

Accidental poisoning of children at home, starting point of drug abuse by teenagers at home and uninformed self-medication have one thing in common; in all three unused or unwanted medicines are likely culprits. The harm we cause when we fail to properly dispose of medicines we do not need is crippling.
So many people have out of fear or anxiety converted their homes into mini-pharmacies where medicines that are supposed to keep us alive are stocked. COVID-19 worsened this practice and no-bed syndrome also plays a role.
Some of these medications may end up complicating our conditions as we self-diagnose and treat ourselves with what “the all-knowing “social media curb-side doctors prescribe.
From “blood-thinners” including aspirin to steroids, antibiotics, assorted supplements, ivermectin, hydroxychloroquine and even tanks filled with oxygen have found their way into homes. People including children will now “consume” some of these medicines and any left-overs may be accidentally taken, given out to family and friends with “similar” symptoms etc.
We all run the risk of abusing drugs and unfortunately some may end up indulging in “hard drugs.”
Prior to COVID-19 many of us had turned our homes into dumping sites for medicines and we have now expanded our range of supplies. We seem to develop “unholy” attachments to drugs and end up keeping them for years even when they have long expired. I have had several unpleasant requests to identify a drug that is partly decomposed and has no name on its container. Unfortunately I have on all occasions refused to even make an attempt. My trade may teach me many things about humans and medicines but it also teaches me to be wary whenever I attempt to play Sherlock Holmes especially with medicines that are not labelled.
I took another look at “DUMP”, which is acronym for “disposal of unused/unwanted medicines programme.” I must admit I was extremely impressed with the usefulness of the DUMP. Many countries have tried a variety of approaches including self-disposal but I think the option that is being promoted in Ghana by Dr Edward Amporful, Cocoa Clinic and other patrons is exceptional. In my candid opinion every hospital, company and home should adopt this programme.
All you need to do is to return all unused/unwanted or even expired medicines to participating hospitals. Put these medicines in labelled receptacles or bins that are provided. You do not need to disclose your identity, just walk away because your work is done. The necessary arrangements have been made with the relevant regulatory bodies for the safe disposal of such medicines.
Sounds absolutely simple yet this has the potential to save lives; that baby who could have accidentally swallowed some of these medicines is still alive and the teen who would eventually have been hooked on stronger drugs is spared the agony.
I think bins should be in all offices so that staff could drop off their medicines and the appropriate steps taken. Market places could also have these bins available and locked and properly secured to prevent people taking the boxes away. Even homes can have a similar bin for discarding and then periodically taken to participating hospitals/clinics. Unused or unwanted medicines should not find their way into a First Aid Box, they don’t belong there.
How do we amass “riches” in unused, unwanted or even expired medicines?
• We may not adhere to the right dose of the medicine thus we end up accumulating medicines at home.
• Sometimes our healthcare provider may make changes to medicines especially when we have chronic diseases such as high blood pressure but we do not return the old ones to the hospital but instead keep them at home.
• Sometimes we react to a drug and stop taking it, leaving the excess at home. I am not sure why we keep these at home when we are aware we are no longer going to use them.
• …and now we stock medicines for fear that we may not have access to some when we have an emergency. Our excuse is that many people are hoarding social-media proposed life-saving medication. After all we are all still learning.
In support of ‘DUMP’
• A frequent cause of accidental poisoning of children at home is having unused/unwanted or expired medicines within their reach. I have seen children rushed to the emergency room for this reason. Some were lucky to live while others had their exciting life cut short. Start DUMP today and help save lives. Even adults sometimes end up with complications because they assumed a drug was used for something completely different.
• People tend to play doctor or pharmacist at home because they pass on unused medicines to family and friends. This is often the starting point of uninformed self-medication. Many people are unaware that doses and types of medicines needed do not depend only on having an illness that appears similar to what another person on a particular medicine was given.
• When unused or unwanted medicines are improperly disposed of, they may eventually end up polluting water bodies etc. Start DUMP and make a statement on protecting our water bodies.
• Drug resistance is often a consequence of abuse of medicines such as antibiotics and anti-malarias. Kofi starts medicine required to be taken for one week and feels better after three days so he stops. A few days or weeks later Awo appears to have a similar illness so Kofi gives her the medicines left for four days. The process of developing drug resistance has just taken off.
• Keeping expired medicines at home may lead to unsuspecting people taking them and they may end up with additional problems.
• Improper storage of medicines may affect its potency. A typical example is keeping medicine that needs to be refrigerated in a hot room instead. Return these medicines.
We could jeopardise our health or that of others just because we are keeping unused or unwanted medicines. STOP. THINK. JOIN DUMP TODAY! You will be saving lives.
AS ALWAYS LAUGH OFTEN, ENSURE HYGIENE, WALK AND PRAY EVERYDAY AND REMEMBER IT’S A PRICELESS GIFT TO KNOW YOUR NUMBERS (blood sugar, blood pressure, blood cholesterol, BMI)
Dr. Kojo Cobba Essel
Health Essentials Ltd/ Medics Clinic
*Dr. Essel is a Medical Doctor with a keen interest in Lifestyle Medicine, He holds an MBA and is an ISSA Specialist in Exercise Therapy, Fitness Nutrition and Corrective Exercise. He is the author of the award-winning book, ‘Unravelling The Essentials of Health & Wealth.’
Thought for the week –“IN CASE OF AN EMERGENCY you may need someone to be alerted. Since majority of us own cellphones, plan your own rescue by saving this person’s phone number preceded with “ICE.” An example is ICE Kojo Essel.The more people we have who know about “ice” the better for us all. Spread the news!!”
References/Credit:
• Dr. Edward Amporful, Cocoa Clinic.
• www.healthessentialsgh.com

I have over the past two decades looked beyond mainstream medicine to assess other options that lead to holistic health, and I must say it’s been exciting and revealing but it’s not an easy path.
As I matured and my knowledge expanded, I have changed my opinion on some aspects of wellness and many findings have been humbling. We all continue to learn each day.
I will share some of the life-changing skills that we take for granted. In our quest for wellness there appears to be more questions than answers, but moderation still remains key in our daily lives.
The power of prayer, praise and worship of God cannot be taken out of the equation.
Ready. Set. Let us do this together.
- Strength training is a must for ALL of us
- Yes, we all need to dig into the various aspects of exercise; strength training, cardiovascular training, stretches or flexibility training and balance training. If you asked me about a decade ago to pick the king of all exercises, I would naively have answered cardiovascular such as walking, cycling etc. but I am certain now that strength training trumps all and we need to incorporate at least a bit of that in our exercise programme.
- Take a short walk after each meal
- Many of us (your truly included) after dinner barely get to wash our hands before the miracle of the Lotus Eaters sends us to dreamland. Our fingers will be signaling to rats and cockroaches to come out and party.
- Walking a few minutes after eating may hold the key to helping control our blood sugar levels and reduce the spikes in insulin that come with a myriad of issues. At the very least the short walks after eating will add up to increase the energy you expend daily.
- Eating your vegetables and proteins before your carbohydrates may be helpful
- Well, how true may this be? I suggest it is worth trying. I am not saying clear your plate of all protein before you even take a spoonful of carbohydrate. The fibre will slow the absorption of the sugar for hours and even better, you may feel full after the vegetables and protein and not be able to gobble down the mounds of carbohydrates you had planned to dismantle.
- Eat slowly but do not get your boss angry
- Eating slowly does not mean spending hours at lunch and courting the displeasure of your superiors. It takes about 20 minutes for your brain to realise you are full so dear friend, take your time to chew and enjoy your food. A meal “downed” in less than 20 minutes may cause you to virtually suffocate when you top up with water. This is a message to myself and all those who like me eat so quickly that Usain Bolt will envy our speed.
- Eat from small, colourful plates
- Small colourful plates make an impression on our brains. Since the little food appears loaded on a small plate our brains tend to “believe” it’s a lot of food and we feel full for a strange reason. Put the same amount in a large plate and you are likely to be asking for second servings.
- By all means make friends
- The power of social wellness and its role in longevity and an enviable health span is no longer in doubt. By all means make a few good friends and enjoy life! Thank me later.
- Sleep!
- Yes, I do agree there are at least seven forms of rest, and they are all equally important BUT start off with sleep and we will gradually rope in all others.
- Keep your eyes on your numbers
- I have written and spoken about the miracle of knowing our numbers and keeping them in check; blood pressure, blood sugar, lipids and BMI. Today I suggest you look at your heart rate closely. A low heart rate may be an indicator for staying here on planet earth for a long time. Also keeping glycated haemoglobin (long term blood sugar) low is another feather in the cap of longevity.
- Appropriate supplementation
- The golden rule is to get all your nutrients from your food but for many of us that may not be possible hence the need to supplement ( note that supplement overdose does exist)
- It is ideal to discuss supplementation with your healthcare professional and your discussion should look at probiotics, magnesium glycinate, Vit D3 + K2, a good multivitamin and in some instances creatine or whey Protein. I am in no way suggesting you take all these, each individual is unique and that is why it is crucial to discuss your options with a professional.
- Make a conscious effort to be HAPPY
- Happiness affects our entire being in positive ways; smile, say a kind word to someone, be grateful, surround yourself with people who make you happy and not ones who sap your energy, volunteer to support people and by all means get a hobby eg gardening, playing a game etc and the best get news yet; you don’t even have to be good at your hobby to benefit.
We are not waiting for a magical or ideal day to start working on our Health and Wellness, we start today bearing in mind that “the most efficient way to reach our realistic health and wellness goals is to make small healthy choices daily.
AS ALWAYS LAUGH OFTEN, ENSURE HYGIENE, WALK AND PRAY EVERYDAY AND REMEMBER IT’S A PRICELESS GIFT TO KNOW YOUR NUMBERS (blood sugar, blood pressure, blood cholesterol, BMI)
Dr. Kojo Cobba Essel
Health Essentials Ltd/ Medics Clinic
(dressel@healthessentialsgh.com)
*Dr. Essel is a Medical Doctor with a keen interest in Lifestyle Medicine, He holds an MBA and is an ISSA Specialist in Exercise Therapy, Fitness Nutrition and Corrective Exercise. He is the author of the award-winning book, ‘Unravelling The Essentials of Health & Wealth.’
Thought for the week – “WHERE YOU LIVE SHOULD NOT DETERMINE IF YOU LIVE.”- WHO