Health Essentials
Your heart is precious ‘don’t miss a beat’

On September 29 of each year since 2000, we mark World Heart Day without fail but it appears we find a comfortable place to doze off after that, leaving the world’s number one killer to continue its havoc.
This year, the theme “Don’t Miss a Beat” focuses on “the importance of heart and blood vessel (cardiovascular) health by emphasizing how losing someone to heart disease also means losing irreplaceable moments in life. It encourages individuals to prioritise heart health, not to miss important life events, and supports building a world with fewer deaths and more healthy hearts.”
Together with its members, the World Heart Federation spreads the news that at least 80 per cent of premature deaths from heart disease and stroke could be avoided if the main risk factors, tobacco, unhealthy diet and physical inactivity, are controlled.
Stop smoking and prevent others from smoking
a. Once upon a time, puffing the smoke of death was fashionable (maybe from a lack of adequate knowledge?) but certainly in 2025, a healthy lifestyle is in vogue. If you do not smoke, why should you inhale smoke from others (passive smoking)?
Eat more fresh fruits and vegetables
a. In Ghana and other developing countries, we often want something that will fill our stomach and stay there for as long as possible. Why do you think “concrete” is so revered in this great land of ours? Start the day with a hefty dose and top it up with frequent gulps of water. We always come up with 1001 reasons why eating fruits could lead to instant “pocketitis” and may signal the beginning of a third world war in many homes. We love to get into unnecessary arguments about whether fruits should be eaten before or after meals etc., just eat them!
b. We probably should consider buying fruits when they are in season since they are much cheaper at the time
c. Kontomire, cassava leaves and garden eggs, are great vegetables that will not cost you an arm and a leg. You also have the option of cabbage, lettuce etc.
d. The option of having a small garden is great but many of us do not have the luxury of space to do that.
Eat a healthy diet
a. LOW in saturated fats
i. Saturated fats can be found in animal products such as meat, milk, cheese and butter but be careful about plant products such as palm oil. Moderation is ALWAYS key.
b. LOW in refined carbohydrates
i. Our tongues have the power to make or unmake us – talking and eating are two examples of paths that can spell doom. We love sugar, perfumed rice (white), white flour, pasta (macaroni) and white bread and will make excuses to skip brown rice for instance.
c. LOW in salt
i.This is as simple as it is stated. Reduce the salt you put in food. Avoid adding salt to already cooked food. Flee from salted snacks and watch artificial flavouring.
Increase levels of physical activity
a. This is no drill on exercising but sitting on the sofa all evening or sitting at your desk for hours on end has not yet produced a healthy being. Household chores, gardening, walking even if it means while on the phone, using the stairs instead of the elevator all add up. The more you move the better for you. Dear friend, moving the TV remote does not account for much but maybe if you could walk to the TV to change channels or make other modifications then you would be on the right path.
Regular medical examinations to assess heart health
a. Beware of the modifiable risk factors for heart and blood vessels and check them often
i. Uncontrolled hypertension, uncontrolled diabetes, abnormal cholesterol, obesity, physical inactivity and smoking
ii. Get evaluated for sleep apnoea especially if your snore could bring the walls down
Manage Stress
• Check the quality and quantity (duration) of your sleep and rest
• Be happy
• Spend time with people who make you laugh and those who have positive vibes. The pessimists will drain your energy.
Changing these habits and behaviours is possible but we need to be committed. Whatever we are today is by the grace of God and the choices we made before today. Make healthy choices that will protect your heart, and it will continue to perform well for many years to come.
Today many people have died from a heart disease, and others have gained HEART HEALTH, which group would you rather join? Wouldn’t you spend quality time with family and friends for many years rather than being bedridden or spend precious endless hours in hospitals trying to fix our heart and blood vessels.
We have the power to make the right choice and stick to it.
AS ALWAYS LAUGH OFTEN, ENSURE HYGIENE, WALK AND PRAY EVERYDAY AND REMEMBER IT’S A PRICELESS GIFT TO KNOW YOUR NUMBERS (blood sugar, blood pressure, blood cholesterol, BMI)
Dr. Kojo Cobba Essel
Health Essentials Ltd/Medics Clinic
(dressel@healthessentialsgh.com)
Dr. Essel is a Medical Doctor with a keen interest in Lifestyle Medicine, He holds an MBA and is an ISSA Specialist in Exercise Therapy, Fitness Nutrition and Corrective Exercise. He is the author of the award-winning book, ‘Unravelling The Essentials of Health & Wealth.
Thought for the week – “You have the opportunity to have a Heart Health Assessment at The Medics Clinic, Tse Addo from now through Saturday 4th October. Call 055-341- 1221 to set up an appointment or simply walk-in.”
References:
1. World Heart Federation Website
2. The Ten Commandments for A Healthy & Enjoyable Life: Dr Kojo Essel
By Dr Kojo Essel

The call to action
We must move beyond the cycle of temporary outrage. I propose a four-point blueprint for the Ministry of Health and the government: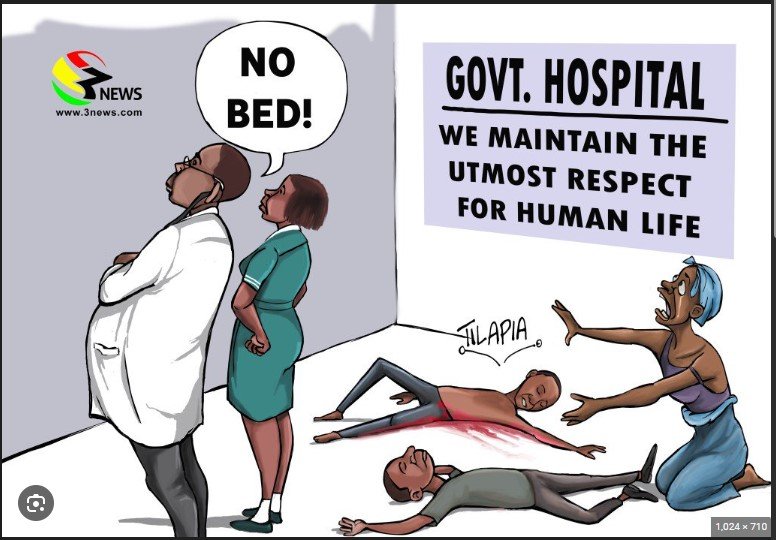
1. A Digital Bed-Tracking Command Centre: Legally mandate all public and major private hospitals to update a live, digital bed-registry every hour. The NAS must be able to see a vacancy before they move. This must be matched with the available resources and services so that the right patient will be sent to the right facility.
2. Strategic Capacity Expansion: We must stop building “prestige projects” and start building high-volume stabilisation centres. We need a targeted investment to triple the ER bed count in Accra and Kumasi within 24 months. This should then be extended to other regional capitals.
3. Specialised Emergency Hubs: Designate specific hospitals as “Centres of Excellence” for Cardiac and Stroke care (and for other health emergencies), ensuring they have 24/7 imaging and intervention capabilities as well as the requisite expertise to manage these conditions. Policy makers must incentivise public-private partnerships to ensure that a heart attack in Accra or Kumasi can be treated with the same urgency as one in New York.
4. Develop a nationwide trauma system: This is extremely important because trauma is a major cause of deaths in Ghana. In the US, each state has a statewide trauma system with three levels. Level 1 trauma centres are usually University Teaching hospitals that provide comprehensive trauma care and also play an important role in local trauma system development, regional disaster planning, increasing capacity and advancing trauma care through research. Level II trauma centres are expected to provide initial definitive trauma care for a wide range of injuries and injury severity.
Level III centres provide definitive care to patients with mild trauma. Having such systems is imperative to ensure proper treatment of trauma patients.
Even for those who survive trauma, disability is a major assault on economic potential and viability. Importantly all this cannot happen with a cash and carry system. Emergencies should be managed under a different model to save life and limb first. Obviously, there is a need to ensure that healthcare facilities will be able to recover their investments in emergency care, and that balancing act needs careful consideration.
Frontline clinicians are often forced to bear the public’s anger for infrastructure deficits they did not create and cannot fix. This is a failure of governance, not a lack of clinical care. Responsibility lies with the policy makers who manage the nation’s resources.
The “No Bed Syndrome” is a systemic disease. It cannot be cured with a directive from the Ministry of Health, parliament or a lecture on ethics. It requires a blueprint, a budget, and the political will to treat this like the menacing threat it is.
It is safe to say that non-emergent healthcare is excellent in Ghana for the most part if you can afford it. However, emergency care is suboptimal. We had a sitting president die from an emergency health issue and a former vice president also die from an emergency. If that is not enough warning, it is clear that anyone can be a victim of an emergency.
If we do not act, the next ambulance driving aimlessly through the streets of Accra could be carrying anyone, including the very people who have the power to fix this issue.
Prof. Jonathan Laryea is a Professor of Surgery at the University of Arkansas for Medical Sciences in Little Rock. Arkansas. He is board certified in General Surgery, Colorectal Surgery and Clinic Informatics.
He is a graduate of the University of Ghana Medical School (Class of 1997)
Health Essentials
Why Ghana’s ‘no bed syndrome’ is a policy failure, not a clinical failure – Part one

OVER the years, No Bed Syndrome has been a major headache in Ghana’s health system. People have expressed different views and today my friend and classmate Professor Jonathan Laryea takes his turn and makes extremely important contributions that should start a deep conversation.
Professor Laryea writes;
Every few months, Ghana wakes up to a familiar, tragic headline. A prominent citizen, a pregnant mother, or a young accident victim has died in the back of an ambulance. They didn’t die because medical science failed them; they died because they spent their “Golden Hour”, the critical window between life and death, touring the gates of hospitals that had no room to receive them.
The public outcry follows a predictable script: anger at the hospitals, calls for “compassion” from doctors and nurses, and a frantic directive from the minister of health and parliament. A few years ago, the directive was simple: No hospital can turn a patient away. The result? We didn’t create more beds; we simply moved the crisis from the ambulance floor to the hospital floor. That also created another outrage.
It is time to stop blaming the frontline workers and start looking at the math. The “No Bed Syndrome” is not a failure of healthcare workers; it is a failure of a country that has not matched its resources to its population growth. Most recently, an engineer lost his life after being involved in an accident. The ambulance drove around for hours before getting to Korle Bu. Though the outcome was sad, I would venture to say that even if Korle Bu had a bed to treat this patient, the outcome would likely have been the same given the time between the accident and when the ambulance got to Korle Bu. When you have a patient exsanguinating, time is of the essence. Even if he got to the right place in time, the other question is would they have enough blood to resuscitate him without requiring family to donate prior to administering the blood?
The impossible equation
Consider the capital city. Accra has a population of approximately 2.9 – 4 million people, depending on who you ask. To serve this massive, high-density population, there are fewer than 400 dedicated emergency room beds across major public facilities.
Let’s do the math: that is roughly one emergency bed for every 10,000 citizens. That is not a recipe for success. When a system is constantly operating at 110 per cent capacity, “No Bed” isn’t an excuse, it is a physical reality. When we force doctors and nurses to treat patients on the floor, we aren’t “solving” the problem; we are compromising hygiene, dignity, and clinical outcomes. You cannot perform a high-quality resuscitation on a crowded floor. This is a capacity issue. We cannot expect this issue to fix itself. There is the need to increase emergency capacity across the metropolis and indeed across the country.
A system in need of coordination
The second failure is logistical. Ghana has made strides in developing a National Ambulance Service (NAS), but we have failed to give that service a “brain” to coordinate it. Currently, an ambulance driver picks up a patient and begins a desperate, manual search for a vacancy. They drive from Ridge Hospital to 37 Military Hospital to Korle-Bu, burning through the patient’s oxygen and time. In an era of digital transformation, it is inexcusable that our ambulances do not have a real-time, cloud-based dashboard showing exactly where the nearest available specialised bed is located. An ambulance without a coordinated dispatch system is just a high-speed hearse.
Beyond the furniture: The “emergency mindset”
A bed, however, is just a piece of furniture if it is not backed by an emergency pathway. The true “No Bed Syndrome” includes a lack of specialised systems. In modern medicine, the “Golden Hour” dictates that, for example:
• For a heart attack: We must be able to perform cardiac catheterization within 60 to 90 minutes.
• For a stroke: We must have the ability to perform a CT scan and administer clot-busting medication within an hour.
In Ghana, if you have a stroke or heart attack, your survival depends more on your luck and your traffic route than on a standardised medical protocol. If a patient reaches a bed but the CT scanner is broken or there is no Cardiac Catheterisation Laboratory or the Catheterisation laboratory is unstaffed/unresourced, the “syndrome” has simply moved from the ambulance to the ward. We have failed to develop the specialized “hubs” required to treat these time-sensitive killers. Accident cases are even worse. The ability to give blood emergently to exsanguinating patients does not exist. Some patients need immediate surgery; for example, patients with gunshot wounds and stab wounds. Sending such patients to a facility where they cannot do emergency surgery is unhelpful.
We must develop a system for triaging patients to the right facilities. There is a need to do a thorough evaluation of our healthcare delivery system and redesign a system that works for Ghanaians. It looks like we have done a patchwork of modifications to what Governor Guggisberg left us and after 69 years of self-governance, we have failed to redesign a system that works for modern-day realities.
Prof. Jonathan Laryea is a Professor of Surgery at the University of Arkansas for Medical Sciences in Little Rock, Arkansas. He is board certified in General Surgery, Colorectal Surgery and Clinical Informatics.
He is a graduate of the University of Ghana Medical School (Class of 1997).



